

Background: Allogeneic stem-cell transplantation (alloSCT) remains the only curative treatment for patients with advanced AML. However, only a minority of these patients achieve disease control prior to transplantation. Natural Killer (NK) cells have potent anti-leukemic activity but are functionally deficient in AML. Adoptive NK-cell therapy using high-doses of functionally active NK-cells could overcome these limitations. We previously developed an ex vivo NK-cell expansion method based on K562 feeder cells modified to express membrane bound IL-21 (mbIL-21) and 4-1BB ligand, (FC21), which resulted in high numbers of hyperfunctional FC21-NK cells with enhanced cytotoxicity and cytokine production. Here we report outcomes of a phase I clinical trial designed to assess the safety, feasibility and maximum tolerated dose (MTD) of haploidentical FC21-NK cells for patients with relapse/refractory (R/R) AML at MD Anderson Cancer Center.
Methods: Eligible patients were ≥18 years, KPS ≥70 with good organ function. Patients with relapsed AML after alloSCT were eligible if they had no active GVHD and did not require immunosuppression. Haploidentical donors were selected based on KIR characteristics, when multiple donors were available. Donor NK cells were expanded over 3 weeks and cryopreserved. Three dose levels between 106-108 cells/kg were planned. Patients received cytoreductive chemotherapy with fludarabine 30 mg/m2/day and cytarabine 2 g/m2/day for 5 days (4 days for age >60) and G-CSF (subsequently eliminated). 3-7 days after chemotherapy, patients received FC21-NK cell infusions 3 times per week, up to 6 infusions.
Results: As of 4/14/2020, 15 patients were screened, 12 of whom were eligible and received the FC21-NK cells. Median age was 60 years (range 25-70); 6 (50%) had adverse cytogenetics, 8 (66.7%) had adverse ELN genetic risk, 6 (50%) had primary induction failure, 2 (16.7%) had CNS disease and 4 (33.3%) had secondary AML. Median number of prior treatment regimens was 5 (range 2-8), median blast count at enrollment was 47% (range 7-88).
Median time from diagnosis to enrollment and to first NK-cell infusion was 16.6 (range 2.5-98.1) and 17.2 (range 3.1-98.6) months, respectively. Donor-recipient NK-cell alloreactivity was seen in 5 patients (41.7%). Median number of NK-cell infusion was 6 (range 3-6); 8 (66.7%) and 4 (33.3%) patients received NK-cell dose of 1 X106 and 1 X107 cells/kg, respectively. MTD was not reached. Seven patients had ANC recovery post-NK cell infusion with cumulative incidence (CI) of ANC recovery to 500/mm3 at 60 days of 58.3%. Eight patients (66.7%) achieved complete remission (CR) (N=4, 33.3%) or CR with incomplete hematologic recovery (CRi) (N=4, 33.3%) at 30 days post-NK cell infusion. One patient with CR had negative minimal residual disease (MRD). Five patients (41.7%) proceeded to haploidentical alloSCT from the same donor and were transplanted in CR/CRi, all but one with persistent MRD.
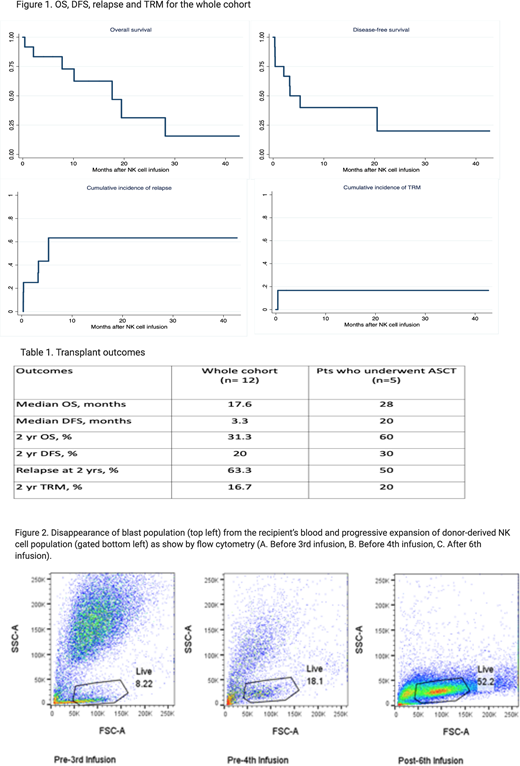
With a median follow-up of 13 months (range 4.1-42.7), median OS and DFS were 17.6 and 3.3 months, and 28 and 20 months for patients receiving alloSCT, respectively. Other outcomes including 2-year OS, DFS, relapse and TRM are shown in Figure 1 and Table 1. No infusion related toxicity or cytokine release syndrome was observed. Two patients were evaluable for FC21-NK cell persistence with haplotype-specific anti-HLA antibodies. FC21-NK cells were detected 5 and 6 weeks after the last FC21-NK cell infusion, respectively. A progressive decrease of the blast population with progressive expansion of the FC21-NK cell population after repeated NK-cell infusions was noted in samples collected from one pt (Figure 2). Persistence is also being evaluated by STR chimerism.
Conclusions: Multiple infusions of FC21-NK cells yielded unprecedented outcomes with 66.7% of patients responding and approximately half proceeding to alloSCT in a heavily pre-treated, ultra-refractory, high-risk patient population. Responses were observed irrespective of dose. FC21-NK cell therapy was very well tolerated with no attributable AEs and were shown to persist for at least 5 weeks after infusion. These encouraging results warrant further clinical evaluation of FC21-NK cells in R/R AML patients.
Ciurea:Kiadis Pharma: Current equity holder in publicly-traded company, Research Funding. Schafer:Kiadis Pharma: Current Employment. Shpall:Zelluna: Membership on an entity's Board of Directors or advisory committees; Adaptimmune: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; Magenta: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; Takeda: Other: Licensing Agreement. Konopleva:Calithera: Research Funding; Eli Lilly: Research Funding; Kisoji: Consultancy; Reata Pharmaceutical Inc.;: Patents & Royalties: patents and royalties with patent US 7,795,305 B2 on CDDO-compounds and combination therapies, licensed to Reata Pharmaceutical; Forty-Seven: Consultancy, Research Funding; Sanofi: Research Funding; AstraZeneca: Research Funding; Agios: Research Funding; Ablynx: Research Funding; AbbVie: Consultancy, Research Funding; Ascentage: Research Funding; Rafael Pharmaceutical: Research Funding; Cellectis: Research Funding; F. Hoffmann La-Roche: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; Amgen: Consultancy; Stemline Therapeutics: Consultancy, Research Funding. Lee:Kiadis Pharma Netherlands B.V: Consultancy, Current equity holder in publicly-traded company, Membership on an entity's Board of Directors or advisory committees, Patents & Royalties. Champlin:Actinium: Consultancy; Johnson and Johnson: Consultancy; Omeros: Consultancy; DKMS America: Membership on an entity's Board of Directors or advisory committees; Cytonus: Consultancy; Genzyme: Speakers Bureau; Takeda: Patents & Royalties.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal